By Jack Winsdor, repost
Ohio Governor DeWine, Director of Health Acton and Lt.
Governor Husted started handling the Coronavirus outbreak with faulty modeling,
while ignoring critical real-time data. Now the trio suppresses critical data.
Ohioans: aware, enraged and bracing to fight for the truth.
The backdrop: COVID-19 first made an indelible mark on Ohioans when
Governor Mike DeWine canceled the 2020 Arnold Sports Festival, which was
schedule to start March 5.
On March 16, Governor DeWine backed a lawsuit seeking to
postpone the primary election scheduled for the next day. The suit was filed by
Ohioans who feared voting in person would expose voters and poll workers to
COVID-19.
Franklin County Common Pleas Judge Richard Fry declined to postpone
the election, but Fry’s decision did not stop DeWine. In the late hours of
election eve, Ohio Department of Health Director Amy Acton declared a
healthcare emergency to force polls closed. The emergency powers are granted by the
Ohio Revised Code and have been in effect since March 16.
On March 23, DeWine announced a two-week shelter-in-place
plan, made legally binding by Acton’s emergency order. By that date, the world had
seen horrifying videos and read data on the COVID-19 outbreak in northern Italy.
If the Governor’s announcement and citizens’ compliance
constitutes a social contract, as DeWine has said in press conferences, then that
contract was inked on March 23, 2020. DeWine promised to make decisions based on the
best science, medicine, and data, and to deploy all necessary resources to flatten
the curve and ramp hospital capacity. DeWine and his team also pledged to be
transparent with data. Ohioans committed to stay home to flatten the curve and buy
hospitals time.
Early data flawed
Nearly a week before the stay-at-home order was issued, Imperial College
epidemiologist Neil Ferguson modeled the COVID-19 outbreak. Ferguson’s model became
the point of reference forleaders across the globe, influencing lockouts and
sheltering policies.
Ferguson himself backtracked on his model’s accuracy just
weeks later after the projections tanked. The swing and miss on COVID-19 is not
Ferguson’s first projection whiff. Ferguson predicted 200 million would die from the
bird flu in 2005-deaths totaled 455. In 2009 Ferguson predicted 65,000 people would
die in the U.K. from swine flu—the death toll was 392.
Ohio Department of Health (ODH) Director Amy Acton delivered
early projections and modeling based on Ferguson’s wildly inaccurate Imperial
College model. Acton guessed 100,000 Ohioans were already infected when she
introduced her modeling. She also projected the
COVID outbreak would peak in April and overwhelm hospitals, produce 62,000 new cases
a day and infect 40% to 70% of Ohioans. Like Ferguson’s model, Acton’s projections
were exponentially inaccurate.
The ODH model was revised twice, the first time revising new
cases per day to 10,000, the second revision ratcheting new cases down to 2,000 new
per day. Outside of sampling a full prison with thousands of inmates, Ohio has never
seen more than 100 cases in any given day throughout the health emergency.
Where Acton erred on projections, Ohioans extended grace
because COVID-19 was pitched as a novel virus without clear data on contagiousness,
how it spreads, who is at risk and how many people would need hospital and intensive
care.
Up-front information did exist—information directly related
to COVID-19, and studies related to the secondary impact of shut-it-all-down
policies.
Early data ignored
Whether willfully or ignorantly, important information was ignored.
The information that could have been used to direct public policy and
mitigation strategies.
Information out of Italy and China revealed two critical factors DeWine and Acton
could have used to laser-focus their response to Coronavirus: 1) people aged 79 and
older with other diseases are most at risk for serious health outcomes, especially
death; 2) People above 30 with high blood pressure, diabetes and heart disease were
at accelerated risk, though much lower than risks to the age ranges 60-80 years and
older. No one below 30 died from Coronavirus.
This information was clear even before Ohio Department of
Health Director Amy Acton signed the first stay-at-home order.
The perils of economic fallout and sheltering-in-place were
also documented for consideration as the administration formed policies.
After the first SARS outbreak, Studies on the secondary impact to mental health
showed serious distress among those quarantined, causing PTSD and depression when
the sick were quarantined for just two weeks or less.
The 2008 financial crisis spiked suicides due to unemployment: rates were four-times
higher; a 1% increase in unemployment resulted in a 1% increase in suicides among
males.
Instead of using a scalpel to carve-out policies to target the most vulnerable,
alleviate economic impact and spare the uninfected from
sheltering, DeWine, Acton and Husted did the opposite—they swung a wrecking ball.
What we know today about COVID-19, we knew in March. Regardless, Acton, DeWine and
Husted implemented draconian measures and then defended their decisions by marketing
the doom and gloom from the Spanish Flu pandemic, which happened over 100 years
earlier.
Acton shared a tale of two cities: Philadelphia and St. Louis. Philadelphia was not
as diligent about sheltering, resulting in higher
infections and deaths. St. Louis was compliant and produced fewer infections and
deaths. Ohioans were encouraged to be like St. Louis.
According to the CDC, sheltering-in-place, social distancing, disinfecting, and
practicing good hygiene made sense in 1917—it was, essentially, all the world had to
combat the H1N1 outbreak. Influenza vaccines did not yet exist, nor did antibiotics
for secondary infections (secondary infections drove the second surge of the Spanish
Flu). Pharmaceutical interventions for therapy also did not exist.
The Spanish flu killed children under five (5), healthy
adults aged 20-40 and elderly over age 65. A much larger percentage of the
population was at risk of death during the 1917 pandemic than people in 2020exposed
to COVID-19.
Technology, communication, vaccines, therapeutic drugs and
overall healthcare have made leaps and bounds forward since 1917 and have
enabled us to better navigate the dangers of a pandemic.
We did our part
If early models and comparisons to the 1917 pandemic did
anything to Ohioans, they manipulated emotions and produced compliance. And perhaps
that was the intended consequence.
People stayed home. Owners of nonessential businesses
voluntarily walked away from livelihoods. Employees worked from home, while caring
for their kids and becoming their ad hoc teachers. More than a million people
accepted unemployment and waited, patiently, for the Ohio Department of Job and
Family Services to catch up.
Hospital capacity, ICU capacity and positive cases never
came close to embarrassingly inaccurate projections. The health system we set out to
save by flattening the curve has actually been negatively impacted—the broad
cancellation of all “elective procedures” including things like cancer screenings
has led to furloughs, layoffs and loss of healthcare capacity due to the economic
consequence of not having enough patients—COVID or otherwise.
Plus, there is a broader health consequence to the mental, emotional and
physical health of Ohioans that is just now starting to be understood.
Much has changed since March 23. One thing has not: DeWine’s
commitment to draconian measures in the face of civil opposition and
contradictory data. DeWine decided to double down on the measures and vehemently
rejects input that goes against his administration’s models, ideas and policies.
Legislators stepped up opposition to Governor DeWine during
an April caucus call. According to two legislators who wished to remain
anonymous, DeWine was not only closed to different views, he was defensive and
volatile, yelling at the elected officials. At one point he shrugged off questions
and opposing data as conspiracy theory.
In early May, amidst rapidly growing economic distress and
civil dissension, the Ohio General Assembly and Senate began drafting
legislation designed to limit the Health Director’s powers to 14 day before
involving the legislature. Legislation also sought to reduce fines and criminal
penalties waged against people who defy Acton’s orders. Senate Bill 1 and Senate
Bill 55 were subsequently drawn up, but even before they reached a vote, DeWine
threatened to veto any legislation designed to limit Acton’s authority.
Suppressed data: Daily death totals
During each presser, Amy Acton will review the Ohio COVID-19
dashboard. You may note that Acton reports deaths as “deaths reported in the last 24
hours.”
Deaths reported in the last 24 hours are different than the actual number of deaths
in the last 24 hours. The number reported is almost always inaccurate and inflated
because it includes deaths over several days, perhaps as far back as January.
The practice of using “reported” data causes the public to perceive more cases and
more deaths than are occurring in the present. The practice is confusing the press,
the public and at times even the Governor and
Dr. Acton seem confused.
On May 23, the Ohio Department of Health indicated there
were 84 reported deaths over the past 24 hours. However, the real number
of deaths totaled seven (7), a difference of 77.
This 77 death inaccuracy was found only after reviewing the CSV file available for
download on the state dashboard site The CSV file lists the accurate daily number of
deaths—and can be found after much digging.
Suppressing the daily death totals is dangerous. Inflated and inaccurate data gets
picked up and reported by unsuspecting news outlets. That, in fact, happened on May
23 when an Ohio media outlet reported the 84 deaths under the headline: Deaths more
than double the previous 24-hour period.
Misrepresenting the death total is not a new practice.
During a press conference on April 14 Governor DeWine repeatedly claimed 50 people
died over the previous 24 hours. The actual number of reported deaths was five (5).
When confronted with the disparity, DeWine deferred to Amy Acton who said, “I think
it might be a reporting lag.”
R-naught of COVID-19 in general population
The r-naught factor is a number indicating viral infectiousness. The r-naught (often
expressed as R0) tells you how many people will, on average, be infected by one
infected person. For example: if COVID-19 had an R0 of four, one infected person
would, on average, infect four other people.
The r-naught of COVID-19 has become a data point of interest
during Governor DeWine’s daily pressers. Acton projects COVID-19 had an original
r-naught of between 2.5 to 5.0. Acton and DeWine reported a current r-naught of 1
during one press conference and .8 during another.
DeWine warns if the r-naught ascends above the 1.0-1.2 range, it will set off alarm
bells. Translated: an r-naught above 1.2 could trigger
a rollback—shuttering businesses, locking Ohioans out of public spaces, further
slowing a re-opening, while increasing pressure to comply with backdoor controls
such as testing and contact tracing.
Given the importance of this measure, it makes sense to dig
into how it is reported. Not every part of the state has the same demography,
population density, and the potential for a high secondary surge. The now famous
ping pong ball commercial is a powerful visual, but it is based on faulty
assumptions.
The video shows how one infection sets in motion a massive
chain reaction around you. The problem: not everyone is equidistant from each other;
not everyone will contract the virus; many will not spread the virus; serious
symptoms and death will not result in over 99% of cases, once symptomatic and
asymptomatic infected are counted in the mix. The video is a bogus visual
representation of the spread of Coronavirus.
One solid first step to making the r-naught more meaningful requires
carving-out congregate living data sets. Extracting, measuring and
independently dealing with people who live in these close quarters will produce not
only a more accurate r-naught for the general population, it will also produce
policies that save lives inside prisons, nursing homes and long term care
facilities.
Mixing congregate living with statistics from the general
population skews how infectious the virus may be to the general population. A spike
in congregate living settings could equal a clampdown on the general population—it
would be like punishing the entire class if one child is acting out. Equally
irresponsible: keeping images like the ping pong video and mixed data sets in play.
These serve misinformation and, frankly, panic people.
Common sense can derive that if the current r-naught is 1:1
with mixed data sets, the general population is experiencing a contagiousness that
is a fraction of what occurs in congregate settings. What may be discovered once the
congregate living numbers are backed out is that the r-naught is likely a fraction
of the current 1:1 estimate. And that fractional expression would be a better basis
for mitigation and policy decisions.
On top of separating data sets for congregate living it also
makes sense to look at each of the 88 counties differently—80 of the 88
counties will likely have r-naught values that are miniscule. Consequently,
their differences should be honored with varied policies that apply to people
in those locations.
Nursing home deaths
Just two weeks ago Amy Acton estimated death rates in
nursing homes comprised approximately 20% of the Ohio death toll. As reporters and
citizen journalists investigated that claim, it was discovered that confirmed deaths
were double Acton’s estimate. Continued digging reveals that, as of May 21,
confirmed deaths in nursing homes total 79% of the state total.
The errors seem to stem from mixing data sets, slow responses
and an overall lack of focus on critical information. Failing to dive deep
into
data provided by nursing homes and other congregate care facilities may account for
the utterly irresponsible handling of nursing home infections.
Mixing data sets from congregate settings (information
specific to nursing homes and other congregate facilities) for reporting and
consideration bypassed a crucial step in checks and balances. In fact, the
mixing is a fatal error.
Nursing homes and prisons produce extremely disproportionate
infection rates—and disproportionate deaths in the case of nursing homes. What if
the state would have previously segregated the data sets and treated them
differently—how many lives could have been saved in long term care facilities, jails
and prisons?
The state would be wiser to extract congregate living numbers and to begin dealing
with the disproportionately large number of infections, hospitalizations, ICU visits
and deaths in these congregate
communities.
The slow response to directives can best be seen in the
seven-day delay in DeWine’s response to a directive from Vice President Mike Pence
that called on all governors to perform testing in all their long term care
facilities—all nursing home staff and patients. Pence announced the directive on May
12, but it wasn’t until May 19, a week later, that Governor Mike DeWine took the
initiative to ramp testing in nursing homes—deploying the National Guard to aid in
testing.
In the elderly, the time from COVID-19 onset to death is estimated
at 14 days; seven days is a matter of life or death.
Information on how to best treat nursing home residents who
contract COVID-19 is hotly contested. Kay Ball, PhD, RN, CNOR, FAAN, a 71-year-old
female, contracted Coronavirus despite masking, wearing gloves and following
suggested protocols. Ball’s husband, a 73-year-old male, also contracted COVID-19.
They both recovered.
During an interview, Kay Ball said during her visit to the hospital, the drug
hydroxychloroquine was administered. Ball began feeling better almost immediately.
Bell also pointed out that she received a shot in
her stomach to decrease the incidence of blood clotting; she was also given
zinc and high levels of vitamin C.
Whether there was one treatment, or a combination of many, there seems to be a
growing body of evidence on the efficacy of hydroxychloroquine, zinc and vitamin C.
There is no better time to untangle the facts surrounding the efficacy of
therapeutic drugs and to cut the bureaucracy surrounding their delivery, where
appropriate.
During the May 21 press conference, DeWine, et.al. seemed to
pivot away from primary COVID-19 issues, such as nursing homes, and toward larger
social issues: housing, education and transportation.
The Governor is trying to spin-up an entire social movement
that takes tremendous time, energy, money and effort—and doing it while our
deadliest problem goes largely unaddressed. What is gasping about the
transition to magnanimous social issues is the fact that the nursing home
crisis is condensed to less than one percent of our population; yet it remains a
problem without a solution. Residents in nursing homes are the most immobile in our
communities, they are easily reached, treated and can be saved with a laser-focus.
Instead, we now turn our attention and money to gigantic
initiatives DeWine’s team will try to apply to the 44,825 square-miles
comprising Ohio and its almost 12 million citizens. There may be no bigger sign of
incompetence in our current mindset and decision making.
Antibody testing
In early April, Amy Acton announced the Ohio Department of
Health, with aid from Celexa, would conduct a 1,200-person random antibody test
sample in Ohio. The purpose of the antibody testing was to determine how many
Ohioans have COVID-19 antibodies. This study could potentially tell us much about
how far the virus has spread—especially since we now know it was here in early
January (if not sooner), at a time when there were not mitigation strategies in
place. WMFD-TV has repeatedly requested copies of contracts with Celexa and
information on the antibody testing and information has not yet been provided.
Antibody tests could undermine the perceived severity of COVID-19 in Ohio; tests
could also prove how much more work there is to do to prepare to live with the
virus. Either way, this is either a commitment unfulfilled or information
suppressed.
Average age of death
During nearly every press conference from March through May, Acton would state
“average age of cases was about 50” but she has yet to
publicly say that the average age of death is 81.
Why? A legislator, who wishes to remain anonymous says “they
[Ohio Department of Health] don’t want information that would cause people to not
obey their orders.”
Surface spread and asymptomatic spread Since the beginning of Ohio’s mitigation
efforts, the CDC website has contained information explaining that viral spread on
surfaces may be possible, yet not likely, and not the main way the virus spreads.
Not a single case has been discovered through surface spread; yet Acton took time
during a press conference to inaccurately explain how germs “move” across a counter
top using a swiss cheese mind illustration.
On May 14, the Director’s Dine Safe Ohio Order was issued, extending mandates for
restaurants and bars. In that order was language from the CDC. “The CDC reports that
people are most contagious when they are most symptomatic (the sickest) however some
spread might be possible before people show symptoms although that is not the main
way the virus spreads.”
New studies indicate asymptomatic spread is not occurring.
Instead of discussing the studies and possible implications to our daily
living, the administration continues to double down on masks and other
measures, while trumpeting the message that asymptomatic spread can kill
grandmas and those most vulnerable.
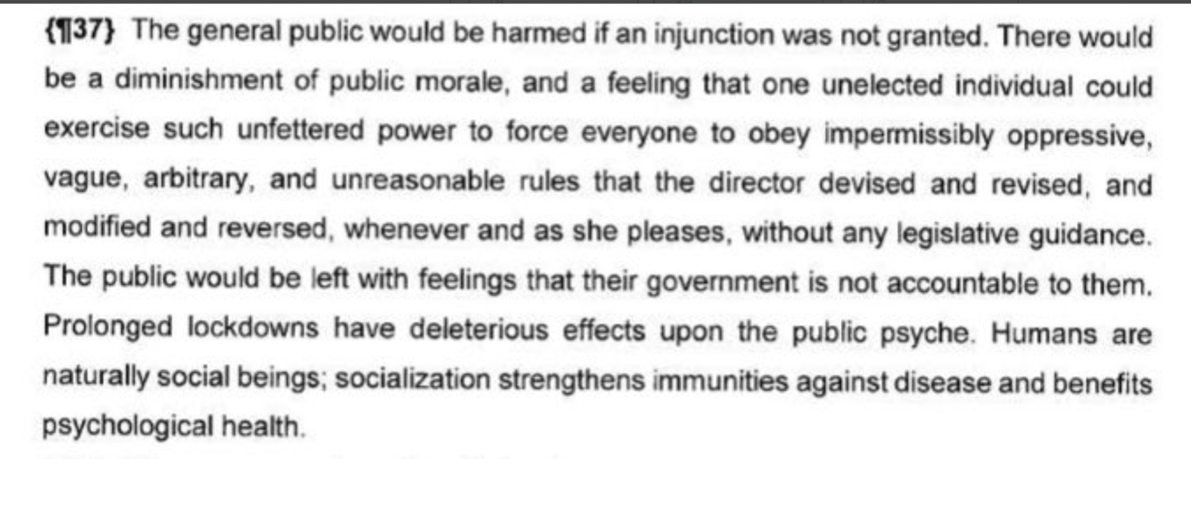
Lake County Judge Eugene Lucci’s decision Lucci’s decision was
treated like anything else that challenges the Governor’s direction, DeWine
downplayed a court decision during
the Thursday, May 21 press conference. DeWine said that all the decision did
was shorten mandates by six days. Common Pleas Judge Eugene Lucci actually said:
“The director (Acton) has no statutory authority to close all businesses,
including the plaintiffs’ gyms … She has acted in an impermissibly arbitrary,
unreasonable, and oppressive manner without any procedural safeguards.”
The judge ruled unconstitutional DeWine and Acton’s rules that shut down
businesses and kept people locked in their homes. The phrase “all businesses” means
just that—all businesses. ntibody testing
In early April, Amy Acton announced the Ohio Department of
Health, with aid from Celexa, would conduct a 1,200-person random antibody test
sample in Ohio. The purpose of the antibody testing was to determine how many
Ohioans have COVID-19 antibodies. This study could potentially tell us much about
how far the virus has spread—especially since we now know it was here in early
January (if not sooner), at a time when there were not mitigation strategies in
place.
WMFD-TV has repeatedly requested copies of contracts with
Celexa and information on the antibody testing and information has not yet been
provided.
Antibody tests could undermine the perceived severity of
COVID-19 in Ohio; tests could also prove how much more work there is to do to
prepare to live with the virus. Either way, this is either a commitment
unfulfilled or information suppressed.
Average age of death
During nearly every press conference from March through May,
Acton would state “average age of cases was about 50” but she has yet to
publicly say that the average age of death is 81.
Why? A legislator, who wishes to remain anonymous says “they
[Ohio Department of Health] don’t want information that would cause people to not
obey their orders.”
Surface spread and asymptomatic spread
Since the beginning of Ohio’s mitigation efforts, the CDC
website has contained information explaining that viral spread on surfaces
may be possible, yet not likely, and not the main way the virus spreads. Not
a single case has been discovered through surface spread; yet Acton took
time during a press conference to inaccurately explain how germs “move” across a
counter top using a swiss cheese mind illustration.
On May 14, The
directors Dine Safe Ohio Order was issued, extending mandates for
restaurants and bars. In that order was language from the CDC. “The CDC reports that
people are most contagious when they are most symptomatic (the sickest) however some
spread might be possible before people show symptoms although that is not the main
way the virus spreads.”
New studies indicate asymptomatic spread is not occurring.
Instead of discussing the studies and possible implications to our daily
living, the administration continues to double down on masks and other
measures, while trumpeting the message that asymptomatic spread can kill
grandmas and those most vulnerable.
Lake County Judge Eugene Lucci’s decision
Lucci’s decision was treated like anything else that
challenges the Governor’s direction, DeWine downplayed a court decision during the
Thursday, May 21 press conference. DeWine said that all the decision did was shorten
mandates by six days. Common
Pleas Judge Eugene Lucci actually said: “The director (Acton) has no statutory
authority to close all businesses, including the plaintiffs’ gyms … She has acted in
an impermissibly arbitrary, unreasonable, and oppressive manner without any
procedural safeguards.”
The Judge ruled unconstitutional DeWine and Acton’s rules that shut down
businesses and kept people locked in their homes. The phrase “all businesses” means
just that—all businesses.
Information is valuable only when it is used
In science an experiment starts with a hypothesis and it is
either proven or disproven through experimentation. True scientists do not mold the
data to a predetermined outcome.
The fact is, after approximately five months of the
Coronavirus circulating in the population, approximately 300 Ohioans have died
outside of prisons and nursing homes, the high majority over 70 years old.
The fact is, asymptomatic transmission is a theory and a
recent study questions whether that theory is true, yet we have never heard
about this study or the CDC announcement that the projected mortality rate for
people under 50 is .0005, or half the mortality rate of the flu.
These things are not conspiracy theories, yet the administration has engaged in the
practice of intentional selection of data to
present to Ohioans—citizens who were promised data transparency and policies based
on the best science.
To be clear: why DeWine is doing what he is doing is
not as important right now as how he is doing what he is doing.
Governor DeWine and Lieutenant Governor Husted often use
sports analogies. In that vein: what makes a great football coach is the
ability to adjust strategy—particularly, the ability to make halftime
adjustments that prepare the team to perform at their highest potential in the
second half.
Great coaches don’t neglect relevant input. Great coaches
don’t double-down on losing game plans. Great coaches don’t study film from a 1917
football game and use the outdated details in the present to call offensive plays
and defensive formations. Great coaches listen to their coordinators and opposing
views.
The first two weeks following the March 23rd shelter-in-place
revealed that 62,000 new cases a day, 40-70% infection rates and overflowing
hospitals were aberrations.
DeWine didn’t adjust. In fact, he tightened the reigns of control and
regulation—exacerbating the crisis.
Since the initial orders, DeWine has paid lip service to
relaxing guidelines and opening the economy but the slow re-opening continues, and
forced compliance for testing and contact tracing now seem tethered to our ultimate
desire to be back to normal.
In fact, the administration has worked overtime to condition
Ohioans to accept a new normal, hinting that there will be no freedom as we
know it until a vaccine is invented and taken. The merits of these issues are
for another article.
To go back to the sports analogy, in the ten weeks since lockout DeWine et.al. have
been beaten by 30 points a game and now stand 0-16
on the season. Meanwhile, robust state programs are being planned for our kids’ fall
education, healthcare, housing, and transportation. This is akin to a winless team
preparing for an upcoming Superbowl.
Deciding what is more offensive is a toss-up. It might be ignoring
a real health crisis in nursing homes and prisons that continues to infect
prisoners and kill our elderly, while choosing initiatives that would be nice to
have. Or, it may be sticking with decisions that will create endless negative
outcomes for people, families, businesses and the economy for years to come.
Why is this happening?
An advisor to the state, who requested anonymity, talked twice with high level
officials inside the Ohio Department of Health and the DeWine administration. On
both occasions, the advisor asked why data is suppressed and presented with a bias
toward worst-case scenarios. On both occasions the advisor was told the message is
packaged and delivered to change how people feel and think about Coronavirus. The
end goal is to build compliance with the new normal.
Perhaps DeWine and Acton are like helicopter parents who are
alarmingly controlling and overprotective of their children. Whatever the reasoning
for their overreach and unconstitutional rules, the unintended consequences of their
actions now threaten to make the cure worse than the virus.
But like stubbornly protective parents, DeWine and Acton may
be hard to redirect. Judge Fry’s court ruling in March was ignored. Judge
Lucci’s order from last week was ignored. The crew continues to ignore data and the
unintended consequences of their policies.
It begs the question: will they ever be held accountable for
their misrepresentation of data? Remember, on March 23 we the people of Ohio
accepted a social contract and we are still waiting for the faithful
delivery—but will DeWine uphold his end of the bargain?
We hear a lot about the new normal. We were doing just fine
with normal: roaring economy, no state budget deficit, kids in school and
protected, living life the way it is intended to be lived—in community.
Now we know that “normal” was happening while COVID-19 was
here from January (if not sooner) to March 23, without: unprecedented numbers of
deaths, overrun hospitals and mitigation strategies to fight the virus.
How does the new normal look? DeWine and Acton are ushering
it in with their masks, social distancing, business mandates, school shutdowns, and
lockouts.
The results: an estimated 2 million unemployed, more than
1,589 nursing home deaths, zero deaths under the age of 30 (but ample
regulations that strap the age group), a startling number of businesses that
will never re-open, and—if history repeats—a 20%-and-counting increase in suicide.
This is Jack Windsor with WMFD-TV in Mansfield. My question
is for the Governor: Sir, when will the administration target real issues
instead of applying a one-size-fits-all approach and crossing their fingers?











 It
appears this decision will make it difficult if not impossible for Dr. Acton to
implement forced closures in the future.
It
appears this decision will make it difficult if not impossible for Dr. Acton to
implement forced closures in the future.




